Ex-Creationist Glen Morton coined the term 'Morton's Demon' to illustrate his mindset when he was arguing as a YEC.
Morton's
demon was a demon who sat at the gate of my sensory input apparatus and
if and when he saw supportive evidence coming in, he opened the gate.
But if he saw contradictory data coming in, he closed the gate. In this
way, the demon allowed me to believe that I was right and to avoid any
nasty contradictory data.
Now, I freely admit that I have my biases. Opponents will say "that's you, that is". Still, I was put in mind of this when - old enough to know better - I got into a lengthy discussion on Twitter with two people who I might describe as 'Covid minimisers'. One in Germany, one in the US, me in the UK (ain't the internet great?). Their basic contention was that the case and death numbers published are artificially inflated in order to stoke fear and justify 'control' of citizens. The fundamental inflationary parameters being
- The use of an unreasonably high PCR 'cycle threshold' in order to generate an excess of false positives
- The coercion or incentivisation of doctors to over-report Covid deaths, whether with or without input from 1 above.
- The deliberate misreporting by statisticians and/or webmasters.
To address 3) first: consistently and undetectably falsifying data is actually quite hard. When people choose figures, they don't mimic real data-generation processes well, and there are statistical techniques one can apply that can detect data-fakery. It is surprising that no-one of a suspicious frame of mind on that side of the fence has attempted to do so.
There is additionally an increasing difficulty in maintaining consilience with independent data sources, and keeping auditors off the scent. It's something we can readily recognise in daily life - lies need more lies to sustain them; eventually they hit upon the hard bedrock of underlying reality. It's much easier to maintain a consistent truth; you are acting with actual states of affairs, not battling against them. Yet this common-sense approach to untruth seems to depart when an idea needs sustenance. Then, the most improbable mass collusion, maintained by shadowy figures with very deep pockets, and a world of complicit actors devoid of integrity, is accepted as probable.
No matter how laboriously one explains the realities of PCR testing or the death certification process, it seems impossible to make headway against this deeply-held belief that Something Is Very Wrong. Morton's Demon won't let you in. Nope: supposedly motivated either by financial reward or fear, a sinister objective - to terrorise the population over a trivial disease, because ... [insert rationale here] ... - is sustained by compliant personnel; not one whistleblower, not one shred of integrity among them.
These supposed global fudgings require a basis; an incentive. If you subscribe to this notion, is the source governmental or corporate? Trump/Biden's America, Ardern's New Zealand, Xi Jinping's China - all want to 'control' their citizens? The latter already does, and they're the most draconian of the lot! It seems elaborate, as hypotheses go. Big Pharma, on the other hand ... its profits are dwarfed by the financial power of most governments. Big Pharma is by no means whiter than white. But - to pick an example at random - from a turnover of $42 billion, Pfizer is supposed to be able to fund operating costs and shareholder payouts and still have enough left over to purchase global test labs, statisticians, national licensing authorities, media both social and antisocial, 'mainstream' scientific publishing, and EveryMedic - even if this action benefits Moderna, GSK or Merck, not Pfizer at all. Hmmmm, I say.
I want my cut, and I want it now!
Enter Malone
Now, no less a personage than Dr Robert Malone has weighed in to reinforce the myth. He's simply regurgitating a trope, not speaking with authority. But while one might forgive amateurs their dug-in heels, lacking a grasp of the technicalities, Malone really ought to know better. In his recent infamous/triumphant (according to perspective) Joe Rogan podcast, he made the following claims:
"So you had a car accident or a bullet to the head and went to the hospital and they tested you with a PCR test that's nonspecific and they ran it up to 42 cycles and they said 'oh look: there's the virus..."
Couple of red flags there. Can you spot them? 😎
Then ...
"... If a patient comes in with a bullethole to the head and they do a nose swab and they come up PCR positive they are determined to have died from Covid .... "
Ummmm ... yeah. Not seeking to influence you in any way, but ... [frantic eye movements; head waggles]. Of course, a layman might think a doctor - especially one published in
molecular biology - must be an expert in PCR. And doctors are bound to
know about death certification, aren't they? Well, not necessarily. Malone does not appear to have seen patients since graduating. These statements indicate clearly either that Malone does not understand PCR and death certification, or he understands them but is deliberately misrepresenting them. It casts significant doubt on either his expertise or his integrity; take your pick. That's an ad hominem argument? Well, tough - what is claiming him to be an authority, if not its reverse?
Let's deal with PCR, and the extent to which data can be fudged by cycle-hacking, first. I already went through the mechanics of PCR in another post; refer to that for a fuller description of the technology.
"Nonspecific"
This one's easy. To call it 'nonspecific', as Malone does, is just plain wrong. Even if not an expert in patient-facing matters, he is a published expert in molecular biology, and he really should know this: one of PCR's great strengths is its specificity.
The specificity of any test is broadly the extent to which it correctly reports samples that
do not contain the item of interest - which is to say, it provides a measure of the proportion of true negatives to false positives. It is generally reported as a percentage, not an either/or. As an illustration, the UK's ONS (Office for National Statistics)
reports that, in a 6-week period when Covid prevalence was low in summer 2020 208,730 tests were performed. 159 of these were positive, giving a
minimum specificity, if they were all false positives, of 99.92%. This is completely at odds with the idea that government bodies are artificially inflating figures, and terrorising the nation by methodological skulduggery -
even with the assumed bias from elevated Ct threshold, the best they can do is find 0.08% false positives as a baseline, which is hardly going to translate into a significant excess of misattributed deaths even if every single false case were mysteriously doomed within the following month.
There are several reasons for false positives; few of which really help the 'inflationists'.
- The test may pick up a different pathogen than that tested for. This is very unlikely with PCR. The primers used are carefully designed to be unique to the genome of interest (although they may or may not distinguish between strains of the same pathogen). But let's say it is picking up something else in large numbers. That simply means it's a pandemic of that 'something else'!
- There may be cross-contamination of actual virus or fragments during the processes of sample collection, transfer and lab handling. These viral fragments still exist, though - the test is correctly identifying them; it is simply not correctly attributing the right individual as the source. But ... where do they come from? If there aren't in fact widespread actual cases, why is there so much environmental SARS-CoV-2 for generation of this kind of false positive? In this instance, such false positives would themselves be correlates of true positivity. The excess they report is always proportional to the amount of Covid about, and so cannot inflate the figures significantly beyond the true caseload.
- The individual may be fully recovered; viral fragments may take up to 90 days to fully clear. Again, this is an example where the test itself is not returning a true false positive - it is not signalling viral RNA which is not there - but it is a false positive case, if we are only interested in current infections. Nonetheless, they were a case, so you're not overcounting cases by including them.
"42 cycles"
A nitpick to start; there's a common confusion between 'cycles' and reporting threshold. A modern qPCR machine runs for a prespecified number of cycles, under user control. That number is typically somewhere between 40 and 45. This is long established practice; if anyone thinks 40-45 was cooked up for the specific purpose of inflating Covid positives, they are mistaken. However, it is not that number of cycles which determines a positive/negative result, but the lower Ct (or Cq): the point at which the detection of fluorescent marker exceeds a threshold. PCR takes time (up to 90 minutes) and reagents cost money; it is not in the interest of labs to run, as a matter of course, way beyond the Ct values that fall in the region of the positive/negative cutoff.
That cutoff itself is not rigid, though. It's not as if 'the Government' (or as Americans like to say, 'the CDC', or 'Fauci') decrees that all Ct's below (say) 43 are to be deemed positive. There is variation between machines, between different primer sets and probes, between different protocols determining the lengths of cycle and temperature (which can themselves be fine-tuned and varied per cycle). Primer and nucleotide concentrations, and the DNA polymerase used, can also have an effect (never mentioned as possible sources of hacking: it's always 'cycles'!)
Look at the graphs in
this paper. It's an evaluation of different kits supplied by manufacturers covering different gene targets (there are
dozens of such papers; just about every nation with the technological resource conducts its own. Makes you wonder why they bother if they're just going to hack it).
These are calibration curves for serial dilutions of known quantities of target sequence. You can run these at the same time as evaluation of an unknown, under the same conditions. Some things to note:
- The exact same dilution, 10-7, reports at Ct35 at top left, Ct40 at bottom right. Which should we use for a rigid positive cutoff? Bear in mind that 5 cycles, at theoretical maximum efficiency, is a 16-fold difference, yet they both report the same initial copy number. It clearly depends on calibration.
- Many runs actually include two or three such gene targets, making a rigid approach to Ct even more nonsensical. If all three report, it does not matter if one of them reports at max Ct; it is virtually guaranteed to be true.
- Even at 40, the value fits quite neatly on the best fit line. This isn't a true guide to false positives - you'd need many more replicates - but it does indicate that, even at Ct40, the test is not going haywire due to 'too many cycles'. The amplification is directly proportional to what is known to be present. If high cycles generated 'phantom amplicons', the graphs above would be curves, steepening to the left.
After the preset number of cycles, if no Ct value is returned, that is reported as a negative sample. Included in the run is a 'blank' - a sample with absolutely no DNA/RNA in it. It doesn't matter how many cycles you run for, you will not get a Ct value from a blank - pretty much by definition; the blank is there to verify that spurious positives do not occur. The ability of a blank to act as a control is a demonstration that upping the cycle number does not automatically increase your 'true' false positives - positives that indicate target RNA in the sample where there is absolutely none. So, it is mythical that increased cycles will magic target RNA up out of thin air. They can only amplify what is there.
If you do get a Ct, however, and your controls are all above board and the curve is normal, it is nearly certain that your sample contains your primer targets, in however small a copy number (down to the lower Limit of Detection). But even if a positive high Ct (= low copy number) is returned, it is not necessarily
definitively positive as a case, depending on protocol. If it falls in the uncertain range, it may call for retest, on the same or a different machine, possibly using other primer targets, or a multi-gene set. This significantly reduces the uncertainty; there is much less chance of getting an artefact twice.
Who benefits from a false positive? Let us bear in mind what testing is actually
for. It is not done for any single reason - to 'scare' the populace, say, or soften us up for a subsequent proportionate elevation in death figures. It informs
- Population monitoring
- Isolation
- Contact Tracing
- Ward management
- Clinical management
Much of this demands accuracy, which cannot be sacrificed simply in pursuit of 'desirable' government figures. We might however want to err on the side of caution - viral load is not consistently captured by every swab. Additionally, during the course of an infection, Ct (~viral load) is not static.
i) RNA concentration increases during early infection, as the virus replicates and degradation can't keep up.
ii) It reaches a peak, then
iii) tails off as RNA degradation starts to outpace replenishment from replication.
iv) when viral replication ceases, RNA content diminishes more rapidly, without replenishment.
So:
- If our interest is counting cases, a high Ct, if in stage i, iii or iv, still likely captures a 'case'. It's either going to get lower, or has been lower, and we would be mistaken in rejecting these as cases simply because it is high now. Those high Ct samples harvested at stage ii, peak, conversely, may arguably overcount the mildest cases. The extent to which this is an issue depends on the true proportion of mild cases, but it is hardly going to feed through any major distortion into death stats, since most people won't die of anything in the next 28 days if there's nothing much wrong with them!
- For isolation, contact tracing and ward management, we might justifiably include high Ct's to capture stages i, ii and iii, to avoid the risk of inadvertent infection through mixing. Including iv might be more problematic, but not seriously so.
- For case management, however, we need to include all stages i-iv. A clinician cares less about whether viral replication has ceased, because the most serious reactions are often immune system issues, which can occur postvirally.
There is an ongoing debate as to whether to include Ct threshold in the reported result, additional to the current binary +/-. The WHO are in favour; other bodies, such as the American Association for Clinical Chemistry, are against. This is not from any opposition to transparency, but because of the kind of considerations outlined above. It requires a sophistication in the audience which is not always present - even, by implication, when that audience is the medical profession!
So: even given all those lengthy caveats regarding the relation of Ct to positivity, what do the data say? A
popular pastime here in the UK is importuning the ONS with Freedom of Information requests, clearly inspired by
online Covid scepticism.
"Please provide full PCR test protocol".
"The data I require is as follows [...] PCR Cycle Count, Total Number of Positive
COVID-19 cases".
They try to be helpful:

Note that this is survey data
- random sample testing, not people presenting for testing due to
positive LFT, symptoms, or hospitalisation. Cts may conceivably be pushed
higher (or lower) in those cohorts. But still: 90% of all positives are reported at Cts less than 34 (Column O, gradient-fill green). So even if we discarded all tests giving Ct34 and above - which would be pretty absurd - we would make at best a 10% difference.
The estimated prevalence, meanwhile (yellow column Q), varies sixfold in the snaphot, while Ct changes hardly at all. Thus supposed Ct-hacking does not explain variation in reported prevalence - indeed there is a weak eyeball correlation that shows Ct going down when cases go up. The more common the disease is, the lower the mean Ct needed to detect it - the precise opposite of the expectation if Ct-hacking were driving 'cases'. Also, by some means, cases rise in temperate winters and fall in summers. Are we really to suppose that Ct values are the cause of this? If you want to stoke fear, why allow rates to fall?
These data are also consilient with other measures.
- Lateral Flow Tests, for example, report independently of PCR Ct thresholds.
- Likewise, antibody testing reveals a historic set of infections.
- When reported rates rise, medical staff typically observe an increase in patients with 'classical Covid' symptoms.
- And finally, our own experience can be a guide. Current rates in the UK are about 1 per 15 people, down from 1 in 1,000 last summer. This is affecting train services, bin collection, hospital staffing, and so on, in a manner not normally observed in non-epidemic winters.
"Of course", one might protest. '"it's different in my country". Maybe
so, but the UK data still show a significant infection load, without any
obvious contribution from Ct-hacking. Problems due to Covid are unlikely to be restricted to these islands.
Obviously, I can't go through every country, but to wrap up this section,
here is an example from the US.
Proportionately few cases are reported round Ct40, while we would only remove 25% of cases if we got rid of everything from 35 and up. Which, again, would be be an absurd thing to do; 35-40 is not excessive.
"Shot, but Died From Covid"
It is a pernicious myth that anyone with a positive test is recorded as 'died from Covid'. The myth is not helped by some of the confused/confusing messaging coming out of officialdom, but there is a large group of people absolutely determined to grab hold of the stick by the wrong end, growling at anyone who tries to grab it off 'em!
The basic problem is that causes of death take time to process. There's the paperwork, review with a medical examiner, tests, autopsy, possible interaction with the coroner, data entry; all cause delays of up to a few weeks. The fact of death, however, can be recorded quite quickly. Thus, in order to appease the stats ghouls and publish daily headline figures, a simple intersect of two databases is performed: fact-of-death, and positive-test. In the UK, the cutoff is 28 days for the positive test; a similar cutoff, perhaps varying by a few days, is applied in most jurisdictions. However there is absolutely no intention by this process to prejudice the outcome of the clinical and legal process of certification. It is rough-and-ready. True, it overcounts the shot-in-the-heads (mercifully rare in the UK), the car crashes, etc. But it also undercounts the false negatives; the significant fraction who died untested; those who took longer than 28 days to die.
The myth - the Myth That Will Not Die - is that this intersect is the last word on the matter. Once counted as a Covid death, it is passionately believed it will stay as such right through to the death certificate. Not so.
There are usually two significant parts to a death certificate. Here is the US version; the UK version is broadly similar, since both follow
WHO guidelines
There is simply nowhere here to enter Malone's 'bullet-in-the-head-plus-Covid' situation. Covid would be neither a Cause nor a Significant Condition. There is a grey area: Covid causes neurological issues, so
could be a contributory factor in a fall. But this belongs in Part ll at best. 92% of UK death certificates mentioning Covid have it in Part l - clinical opinion, which we used to trust, held that it was an underlying cause of death. Unless doctors have suddenly lost the ability to diagnose, we should afford them the professional respect to fill these things in honestly, based on clinical presentation and experience, and not simply on a test, or a possible cash incentive (in some countries). If Malone would not falsify for cash, others deserve the same presumption of integrity.
Terminal Covid-related sequelae can be complex. It does not simply result in pneumonia, but - in part due to hyperactive immune response - can also cause circulatory issues, strokes, neurological problems, distributed organ damage. It can sometimes resemble other conditions. This might complicate matters, and here tests help eliminate possibilities. But people haven't suddenly started dying of their comorbidities! Comorbidities render death from Covid more likely.
As above, the Covid-sceptic pastime of ONS-bugging continues apace.
"Can I please request the data on coronavirus deaths from the actual virus and not involved or underlined with a disease".
This fundamentally misunderstands the relationship between comorbidity and Covid. Diabetes and hypertension are significant comorbidities, but people don't typically die 'of' them, but of cardiovascular issues to which the condition predisposes them. Adding Covid to the mix is an added complication, but if they display pneumonia, lung scarring or other organ damage on autopsy, fever, elevated blood markers associated with infection - these are not typical consequences of the comorbidity.
Now, some mortal consequences of Covid - for example a stroke - can also be consequences of hypertension or diabetes. During a Time of Covid, we might put the odd case down to it that should 'really' have gone down to the comorbidity. But if this causes a serious miscount of misattribution, we might legitimately ask ourselves what on earth might be causing a substantial increase in deaths from the comorbidity...
The Bottom Line.
Today (9th Jan 2022), the ONS
reports
- 150,154 deaths within 28 days of a positive test.
- 173,248 deaths where Covid-19 was mentioned on the death certificate.
- 92% of Covid is recorded in Part l, ie as an Underlying (but direct) Cause, giving an adjusted certificated figure of 159,388.
Which is to say, however we count it, there are more attributed deaths than positive tests. So, the doctors have overcooked it! The assumed over-attribution by Ct-hacking has still left us 23,000 cases short; the docs have pulled these cases out of thin air! I'm joking of course; this simply illustrates that it is incorrect to say that Ct values drive the thing, without an overriding clinical opinion.
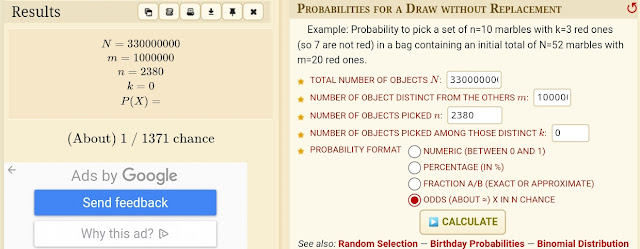
If a test is a false positive, and chance of death is completely uncorrelated, that individual can be assumed to have an average chance of dying in the next 28 days. About 2,000/66,000,000 people die each day in the UK in winter:, a random chance of 1 in 33,000 per person per day. Over the 28 day post-test period, then, an individual has up to 28 such chances of being in that set that day, until they stop being counted. Thus to get just 1 extra death per day from your positive test set, you need about 1,200 false positive tests per day***. If you want to inflate deaths, therefore, Ct is a very weakly-coupled parameter.
*** (That's the arithmetic mean; probabilistically I think you really need the number which
gives a maximal peak for the distribution at k=1, but I'm a maths duffer.
Close enough for jazz, happy to receive instruction!).




Comments
Post a Comment